

Introduction
The COVID-19 pandemic has affected the entire world. Health systems have been affected in such a way that patients with diseases other than COVID-19 have suffered serious consequences. In Latin America, the disease has emerged in a fragile system with more disparities, making our patients more vulnerable. Acute leukemia patients have a high risk of severe COVID-19 disease. Various expert recommendations have emerged with the aim of minimizing the risk of COVID-19 without affecting leukemia-related outcomes. However, multiple logistical issues tangentially associated with the pandemic have also appeared, potentially limiting the quality of management of these patients. The objective of this study was to register treatment modifications associated with the COVID-19 pandemic and its short-term consequences in Latin American countries.
Methods
We included patients older than 14 years, from 14 centers of 4 Latin American countries (Mexico, Peru, Guatemala and Panama), with the diagnosis of acute leukemia, who were on active treatment since the first case of COVID-19 was documented in each country. We documented their baseline characteristics and followed the patients prospectively until July 15, were data-cutoff for this pre-planned analysis was performed. The primary outcome was the incidence of COVID-19 disease and its complications. Secondary outcomes included treatment and consult modifications, and cause of death during the study period. Logistic regression was performed to determine factors associated with COVID-19 and all-cause mortality.
Results
We recorded the information of 635 patients: 58.1% Ph-negative ALL, 25.7% AML, 9% APL and 7.2% Ph+ALL. The median age was 35 years (14-90 years); 58.8% were consideredf high-risk patients. The majority were on CR (68.3%) receiving consolidation or maintenance therapy, while 14.5% were newly diagnosed and 17.2% with relapsed/refractory disease. The majority (91.8%) were treated in centers that were also receiving COVID-19 patients, 40.2% in centers were patients could not be electively hospitalized for leukemia treatment because of the COVID-19 pandemic.
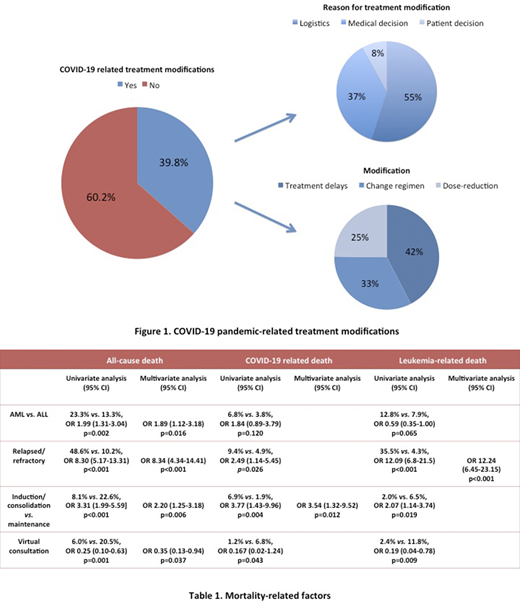
The COVID-pandemic led to treatment-modifications in 40.8% of the cases. Reasons for modifications were associated with logistical issues (22.4%), medical decisions (15.1%) or patient choice (3.3%). The most frequent modification was chemotherapy delay (17.3%) followed by regimen modification (13.4%) and dose-reductions (10.1%). (Figure 1)
83 patients (13.1%) developed COVID-19 disease, the majority mild-moderate disease (54.2%), 27.7% severe disease and 18.1% critically ill; 27.7% required mechanical ventilation and 37.7% died from COVID-19 disease, representing 4.9% of the entire cohort.
We identify as risk factors for COVID-19 disease the presence of active leukemia (newly diagnosed or relapsed) (OR 3.46 [95% CI: 2.16-5.5], p<0.001), high-risk leukemia (OR 1.63 [95% CI: 1.54-4.52], p<0.001) and being treated in a center were elective hospitalization was possible (OR 2.17 [95% CI 1.29-3.67], p=0.004). Treatment modifications, appointment prolongations or the use of virtual consultation were not associated with a reduction in the risk of COVID-19.
On the other hand, 16.7% of patients died during period analyzed due to leukemia (57.5%), COVID-19 (29.2%) or treatment related-mortality (13.2%). Independent factors associated with mortality were AML vs. ALL (OR 1.89 [95% CI: 1.12-3.18], p=0.016), relapsed-refractory disease (OR 8.34 [95% CI: 4.83-14.41], p<0.001), induction/consolidation vs. maintenance therapy (OR 2.20 [95% CI: 1.25-3.18], p<0.001) and the use of virtual consultation (OR 0.35 [95% CI: 0.13-0.94] p=0.037). (Table 1)
Discussion/Conclusions
The COVID-19 pandemic led to significant modifications in the standard of care treatment of patients with acute leukemia. The incidence of COVID-19 disease in acute leukemia patients was considerable and more than a third of the patients with acute leukemia and COVID-19 disease died. Despite a short-follow up, 16.7% of the patients died and leukemia-related deaths were the most frequent. In low- and middle-income countries with fragile health systems, the collateral damage for patients with acute leukemia may be just as important as the direct consequences of COVID-19.
Alvarado:Roche: Speakers Bureau; Novartis: Speakers Bureau; Amgen: Speakers Bureau; Celgene: Speakers Bureau; Alexion: Speakers Bureau. De la Peña-Celaya:Amgen: Speakers Bureau; Janssen: Speakers Bureau; Novartis: Speakers Bureau. Perez:Roche: Speakers Bureau; Celgene: Speakers Bureau; Novartis: Speakers Bureau. Gomez-Almaguer:Amgen: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Novartis: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; AbbVie: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Janssen: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Celgene/BMS: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; AstraZeneca: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Pfizer: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Roche: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal